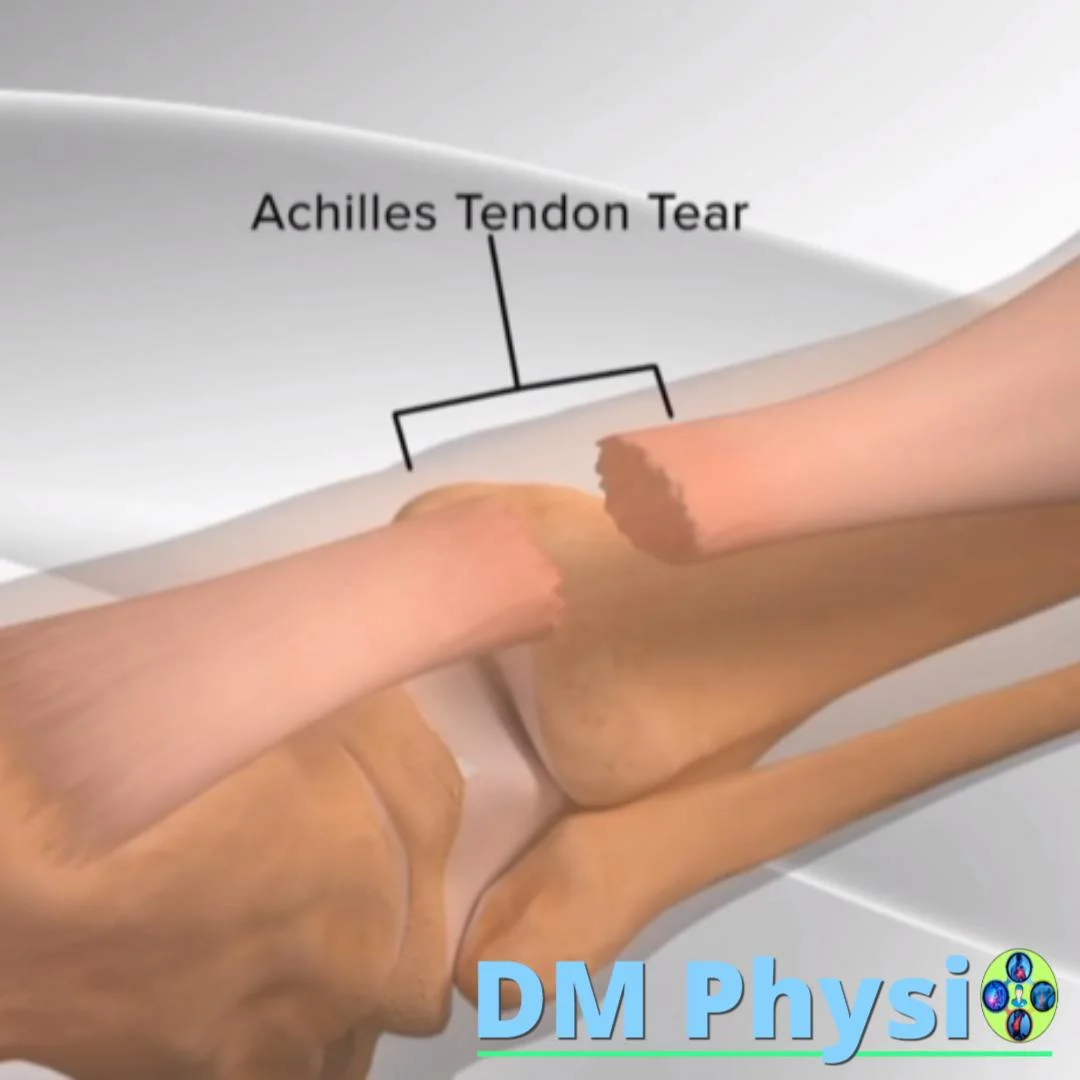
Torn Achilles (Achilles tendon)
It often feels like a sudden sharp pain or an audible "pop" in the back of the ankle or calf, after which walking and standing on tiptoes become very difficult. They appear swelling, sensitivity and often a noticeable "sunk" area above the heel.

What is being damaged and why?
The Achilles tendon connects the calf muscles to the talus bone and transmits force when pushing off. At sudden load (start, jump, change of direction) or on an already overloaded/inflamed tendon, the fibers can tear partially or completely.
Most often the tear is in a "weak zone" 2–6 cm above the heel. Risk factors: unprepared load, sudden return to sports, reduced calf flexibility, chronic Achilles pain, previous injections/medications, and inadequate recovery.
Clinical signs: positive Thompson test (when squeezing the calf, the foot does not point down), a palpable "crack" over the heel and inability to stand on the toes of the affected leg.
Recovery periods: torn Achilles → surgery → physical therapy
Time windows are indicative and are subject to protocol and tissue response.
1) Event: rupture and acute phase (day 0–7)
Sharp pain, often "pop", weakness when pushing off and difficulty walking. Immediately: sparing, lifting, compression, cold applications; immobilization/boot if complete tear is suspected. Next up orthopedic assessment and imaging (US/MRI) to confirm and select treatment.

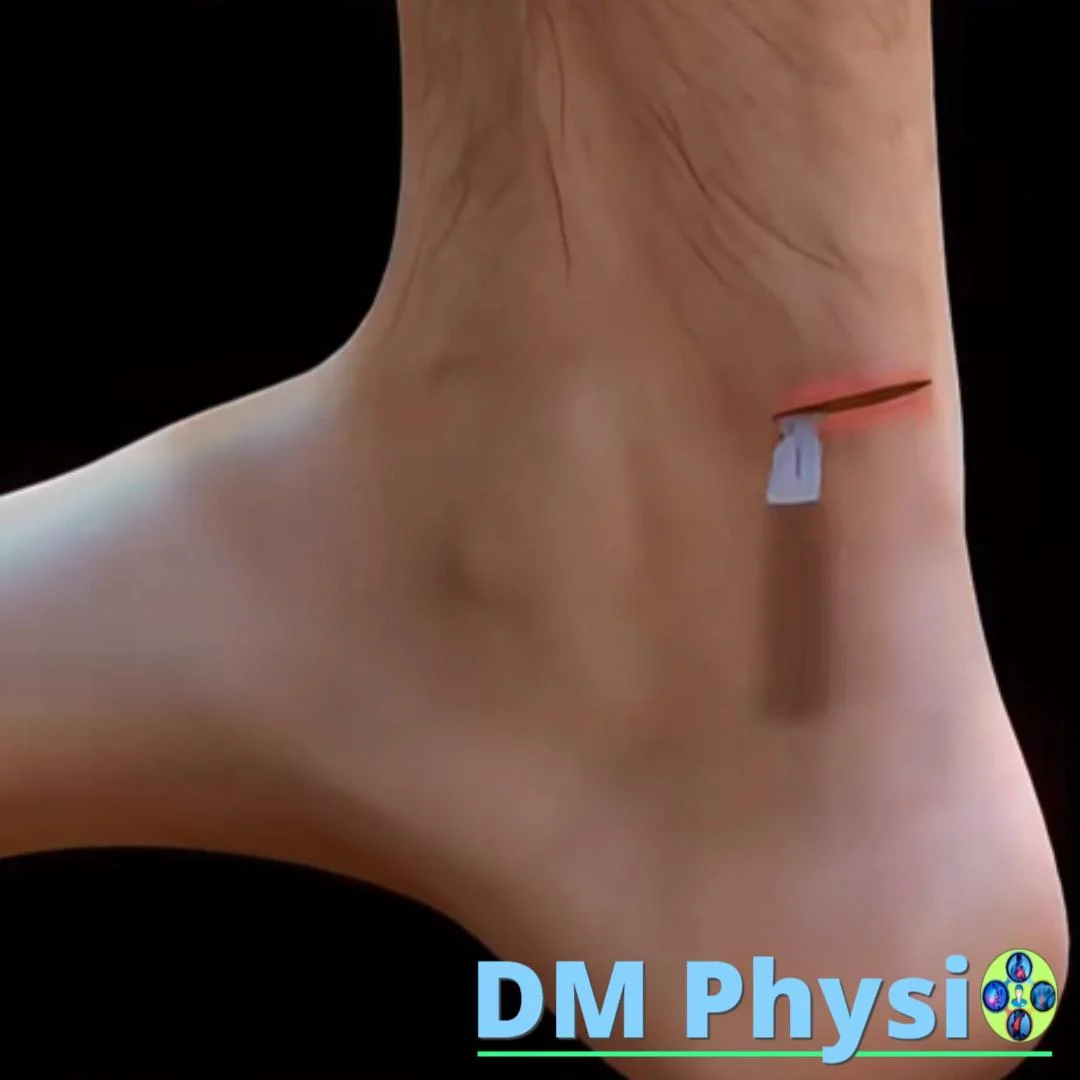
2) Surgery (weeks 1–2) or functional conservative therapy
At complete rupture surgery is usually planned within the first 7–14 days, when the swelling is controlled and the edges allow good approximation. It's an alternative functionally conservative boot treatment and progressive positioning. The choice is individual according to age, activity, distance between ends and goals.
3) Beginning of physiotherapy and stages
After surgery: physiotherapy is usually started in week 1 (day 3–7) with protected active movements, edema control, and gait training with a boot.
Stages in brief: 0–2 weeks – protection and control of symptoms; 2–6 weeks – progressive movement and balance; 6–12 weeks – strength work (concentric/eccentric) and walking without a limp; 12–16+ weeks – running progression, plyometrics, return to sport.

Note: Time windows are indicative and take into account surgical/conservative protocol, tissue response and patient goals.
Physiotherapy - professional plan
Goal: more comfortable walking, restored calf strength, and safe return to activity/sports.
Protective phase (0–2 weeks)
Boot/Brace (optional), dosed loading, elevation and compression sparing active movements in a safe volume, pain free calf isometrics, pelvic/thigh training and gait hygiene.
Movement, Balance and Strength (Weeks 2–8)
Gradual foot straightening according to protocol, active plantarflexion, low resistance elastic band, balance on one leg, normalization of gait (no limp), monitoring: no increasing edema the next day.
Functional loading (8–16+ weeks)
Concentric/eccentric pull-ups, calf endurance, running progression, changes of direction, plyometrics. Return criteria: full more comfortable mobility, strength ≥85–90% of healthy leg, stable walking/running, absence of edema and successful functional tests.