Sprained ankle
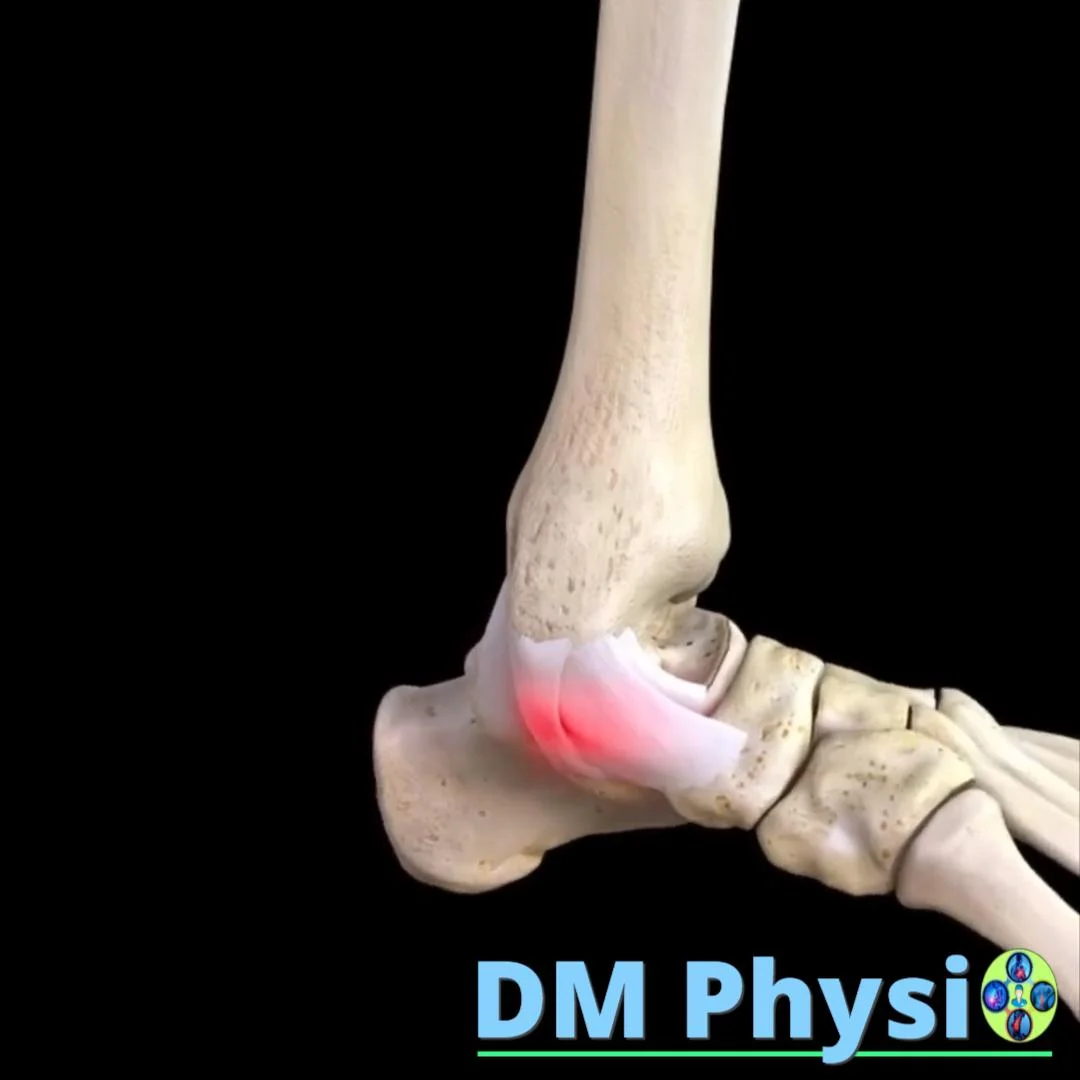
An ankle sprain means overstretching or tearing of the stabilizing ligaments around the joint. It is clinically manifested with sharp pain, rapid swelling within minutes to hours, bruising and feeling of instability when stepping.

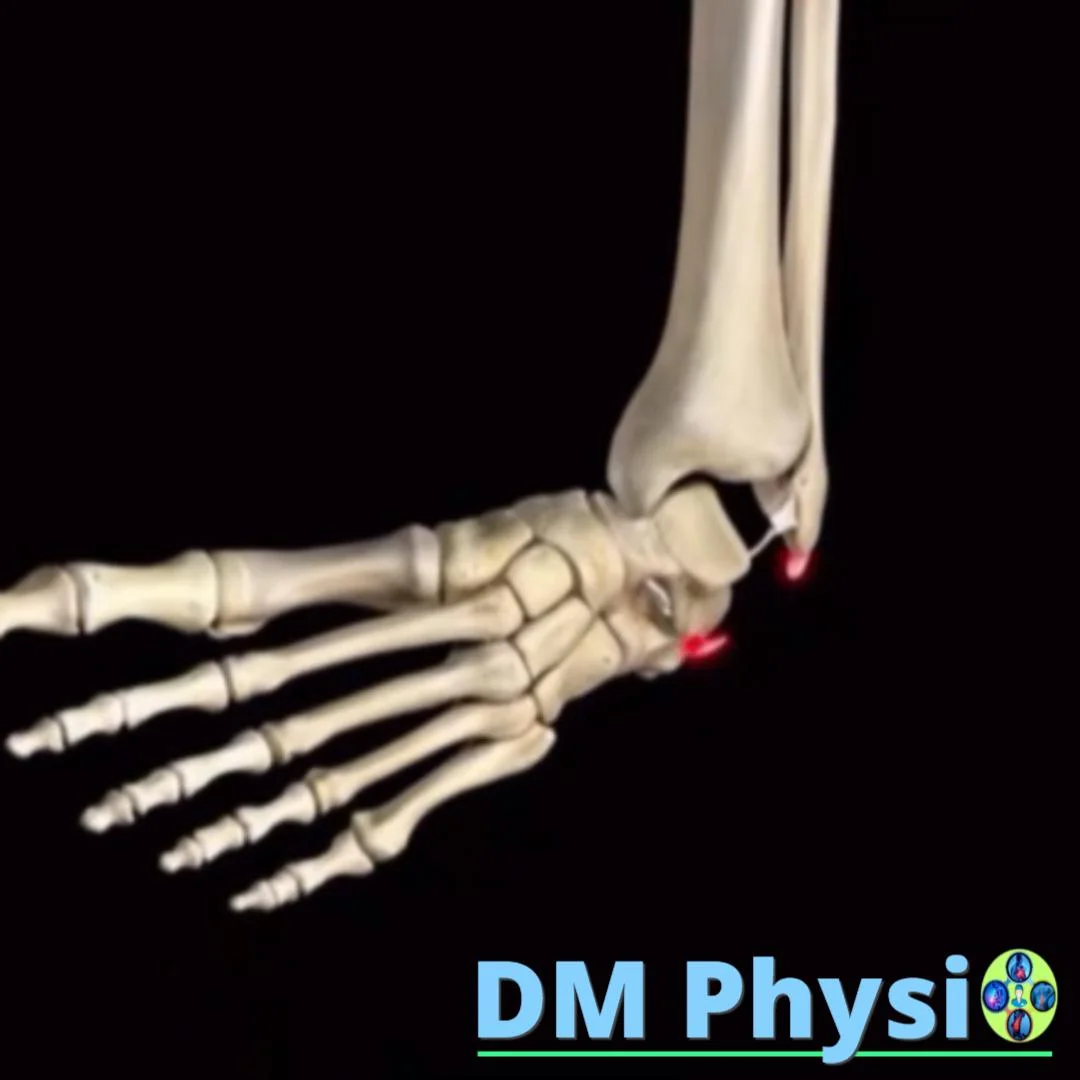
What is being damaged and why?
The ankle is stabilized by strong collagen bands (ligaments), a capsule and an active muscular system. They restrict final and unwanted movements and give the body a "sense of position" (proprioception). At sudden twisting on the foot inwards or outwards the load exceeds the allowable and the tissues are stretched or torn.
When sprained we differentiate three degrees:
— I degree (mild): microtears/stretching, local tenderness, mild swelling, stability preserved; walking is possible with discomfort.
— II degree (medium): partial tear, pronounced swelling and bruising, soreness on pressure and rotation; walking is difficult.
— III degree (severe): significant tear with clinical instability; walking is often impossible in the acute period.
Damage to the outer (lateral) side is most common. Less often, the inner side is affected. The so-called A "high sprain" involves structures above the ankle itself and takes longer to recover from.

What is the most common way to sprain an ankle?
Early and adequate therapy prevents chronic problems and re-injury.
1) Inversion (inversion)
The most common mechanism: rough terrain, poor landing, sudden change of direction. The foot bends inwards, the stress falls on the external stabilizers and a characteristic swelling occurs on the outside.
2) Twisting outward (eversion)
A less common mechanism, often with slipping or direct contact. The internal structures are loaded; the swelling and tenderness are on the medial (inner) side of the ankle and may accompany other injuries.
3) "High" sprain (syndesmosis)
At strong external rotation under load, structures between the tibia and tibia above the ankle are affected. Pain over the joint line, a feeling of instability and difficulty stepping are typical; recovery is longer.

When to see a doctor: visible deformity, severe pain at rest, worsening swelling/bruising or suspected 'high' sprain. Early assessment optimizes recovery.
Physiotherapy and recovery - a professional approach
Goal: more comfortable movement, stability and safe return to activity/sport.
Acute period (0–5 days)
Focus: tissue protection, pain and swelling control. We apply kinesio tape and dosed loading, elastic compression, lifting the limb, gentle active movements in more comfortable volume, isometrics for ankle stabilizers. In more severe cases - orthosis at the doctor's discretion.
Subacute period (1–3 weeks)
Focus: recovery of range of motion, muscle strength and proprioception. We add foot control exercises (pronation/supination), single leg balances, step squats, getting on/off, gait training without a limp. The load is increased according to the reaction (no increase in swelling until the next day).
Functional stage and return to sport
Progression: running exercises, changes of direction, jumps and plyometrics, sport-specific tasks. Return criteria: complete more comfortable mobility, symmetrical strength and stability, absence of edema after loading, successfully passed functional tests (balance/jumps).
Most importantly: Most sprains respond well to conservative therapy. The Sequential Plan (Protection → Movement → Strength/Balance → Functionality) significantly reduces the risk of repeated injuries and accelerates the return to activity.