Temple pain
Find out why it occurs and how to safely manage it.

Why does the temple hurt?
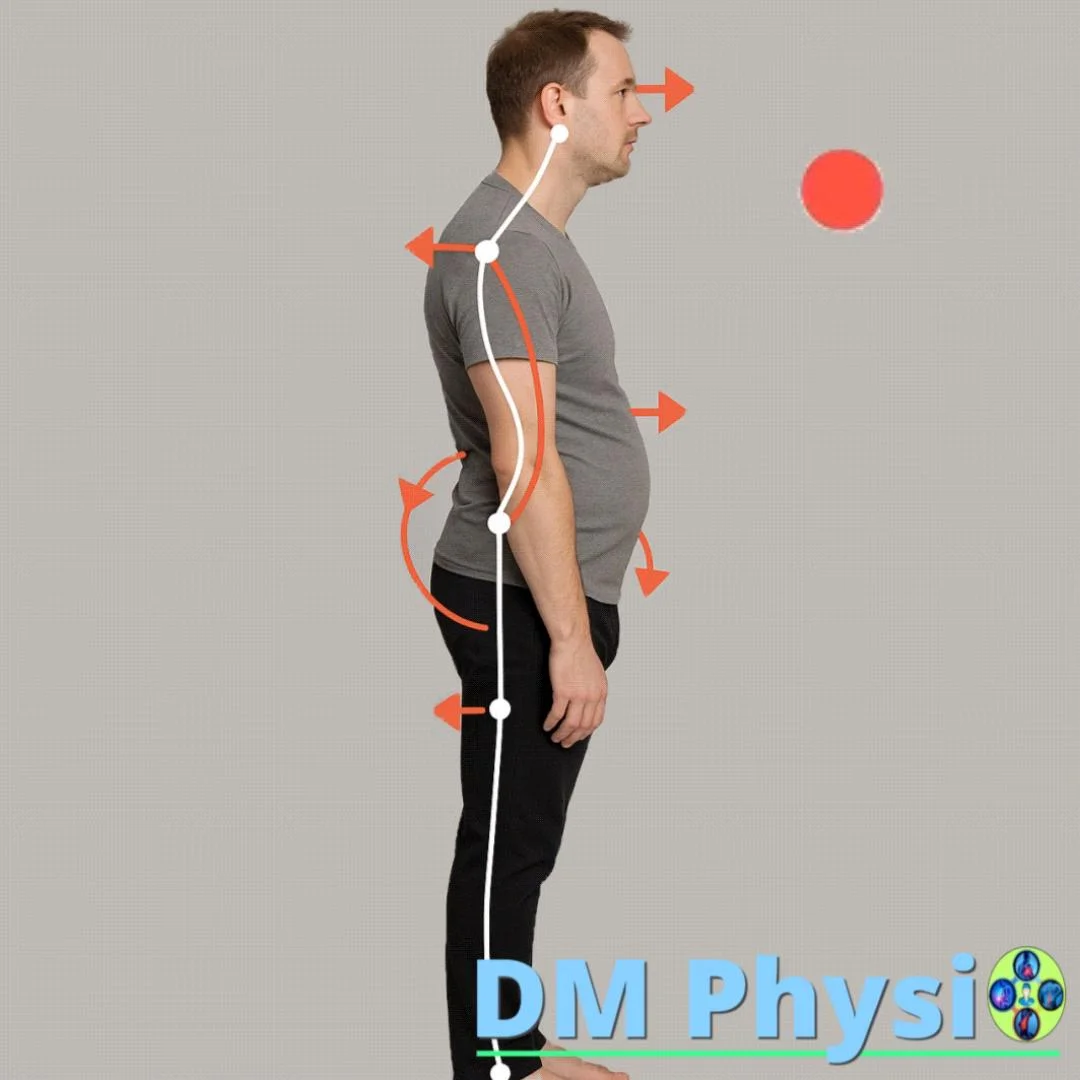
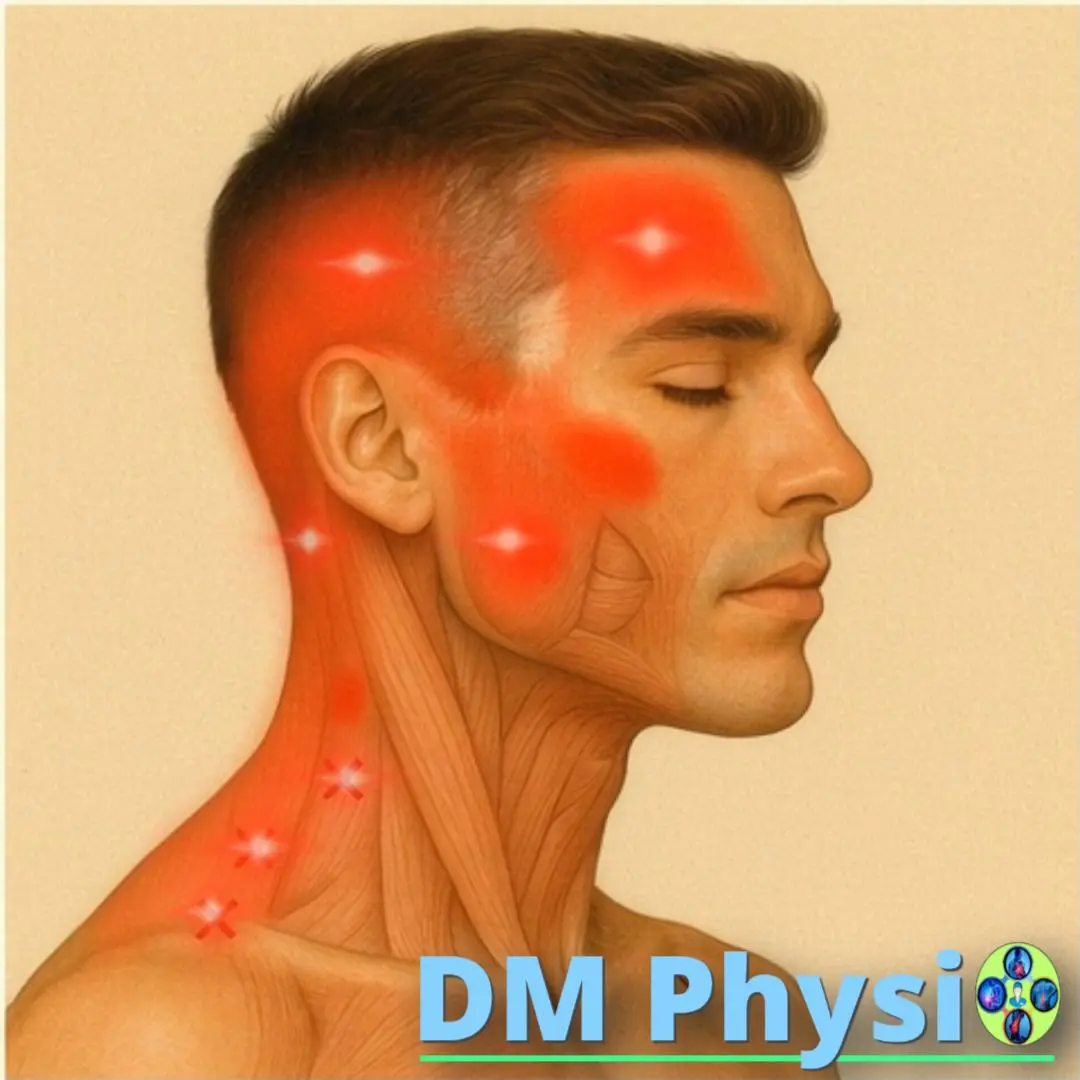
The most common "muscle culprits" are m. temporalis and m. masseter (chewing muscles), as well as neck muscles such as SCM and suboccipitales. When you overstressed from stress, clenching teeth, prolonged sitting or poor position of the head and jaw, they compress the local microcirculation, accumulate metabolites and painful trigger points are activated. The body interprets this as a pressure/pulsation in the temple, often with a feeling of heaviness behind the eye or radiation to the scalp and teeth.
With clenching/grinding of teeth (bruxism) and with "advanced head" in front of the screen, the load on masticatory and neck muscles increases many times.
How and why does inflammation occur?
Three simple steps that explain the cycle of pain.
Sustained tension
Stress, clenching of teeth, long static positions → overstretching of the fibers in the masticatory and neck muscles.
Impaired circulation
Compression of microvessels → less oxygen/nutrients → accumulation of metabolites and hypersensitivity.
Inflammation and pain
Activation of trigger points and spasm → pain in the temple, behind the eye, sometimes a "phantom" toothache.
Which muscles most often give pain in the temple?
m. temporalis
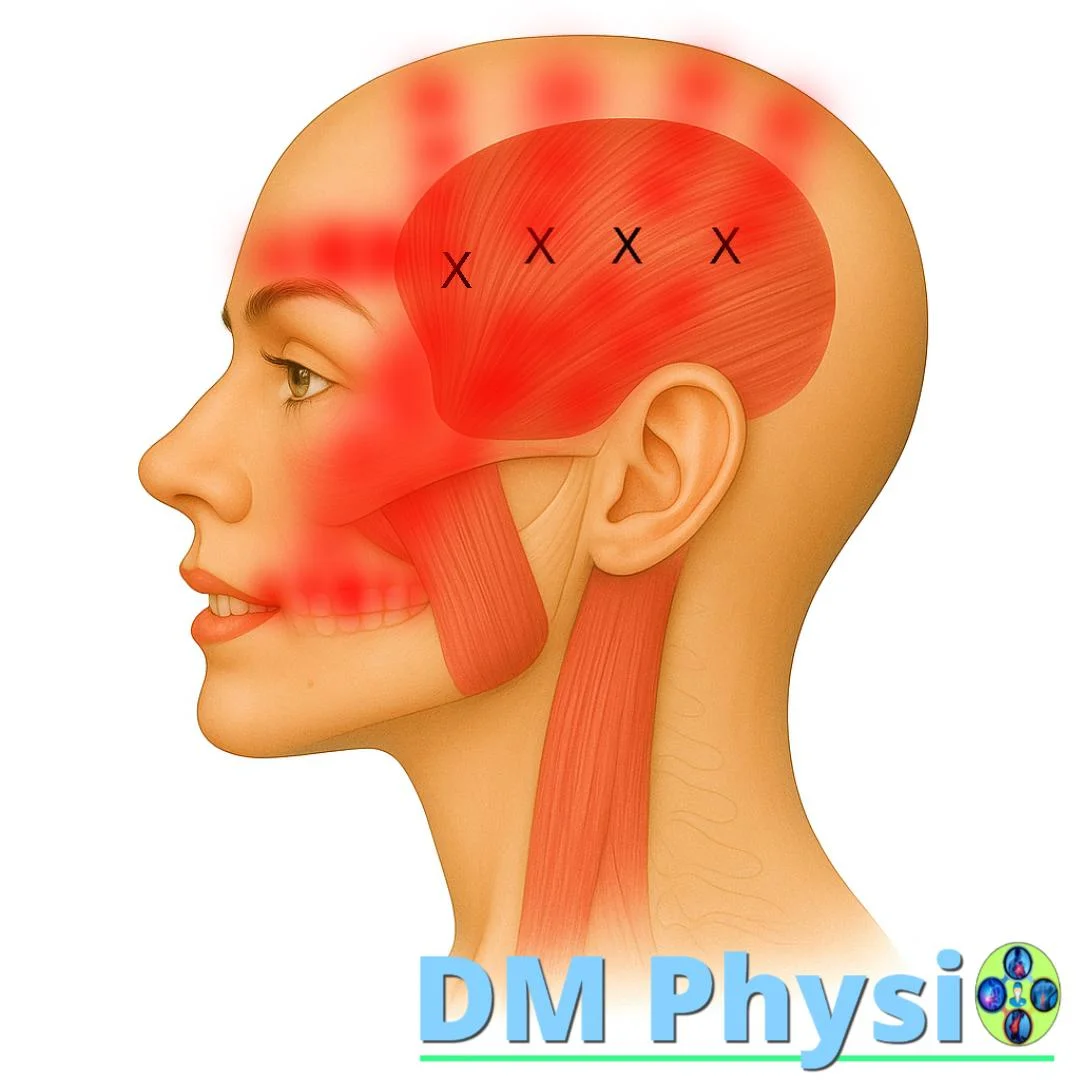
Anatomy and grip
Fan-shaped muscle of temporal fossa; the tendon attaches for the coronal process and the front edge of branch of the mandibula.
Nature of the pain
- Throbbing/pressing pain in the temple
- Irradiation to lateral scalp and behind the eye
- Sometimes referenced pain in upper teeth
m. masseter
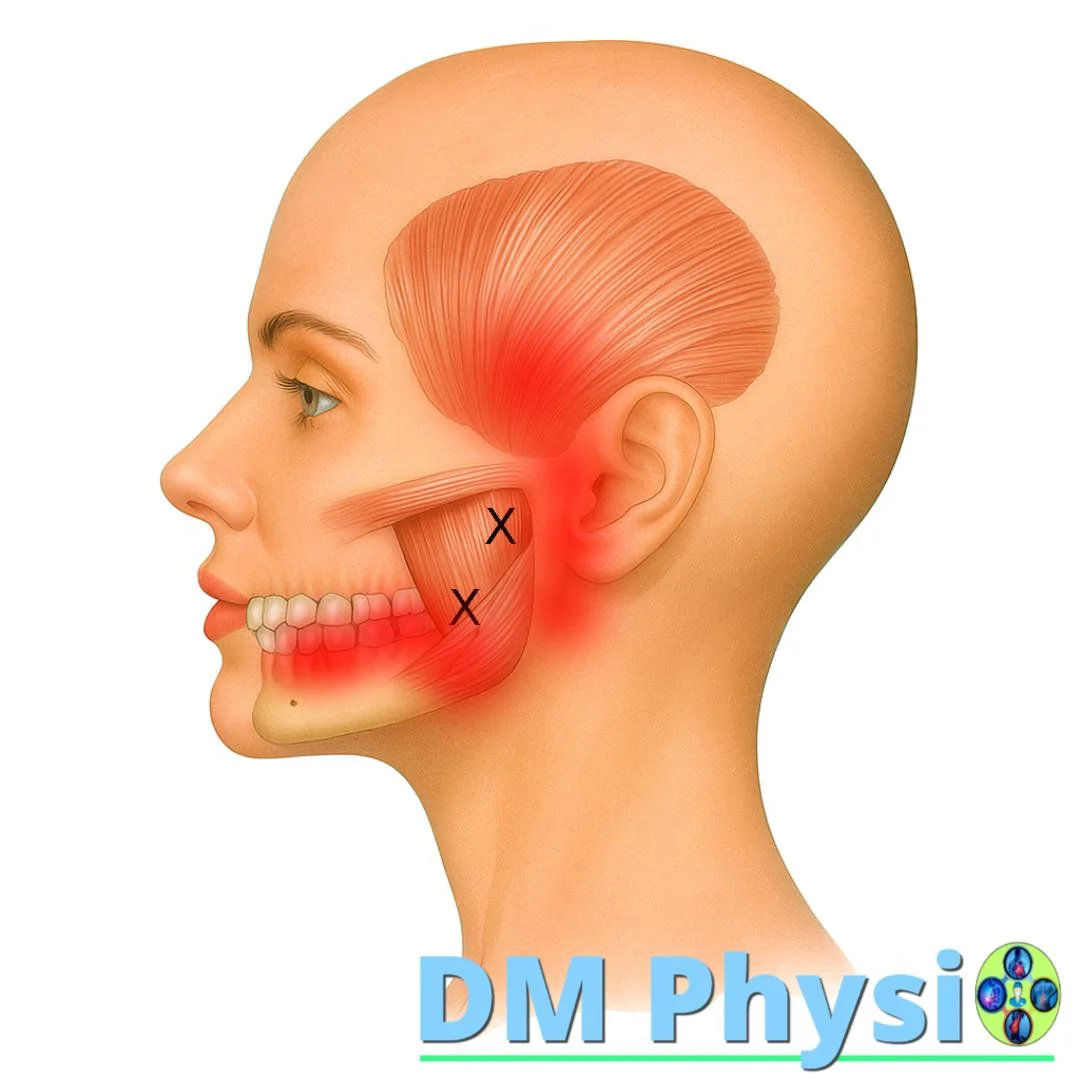
Anatomy and grip
It starts from zygomatic arch and attaches for ramus/angle of the mandible – key to the bite.
Nature of the pain
- Deep pain in the jaw, often mimics a toothache
- Irradiation to ear or temple
- Limited mouth opening; clicking in the TM joint
(SCM) m. sternocleidomastoideus
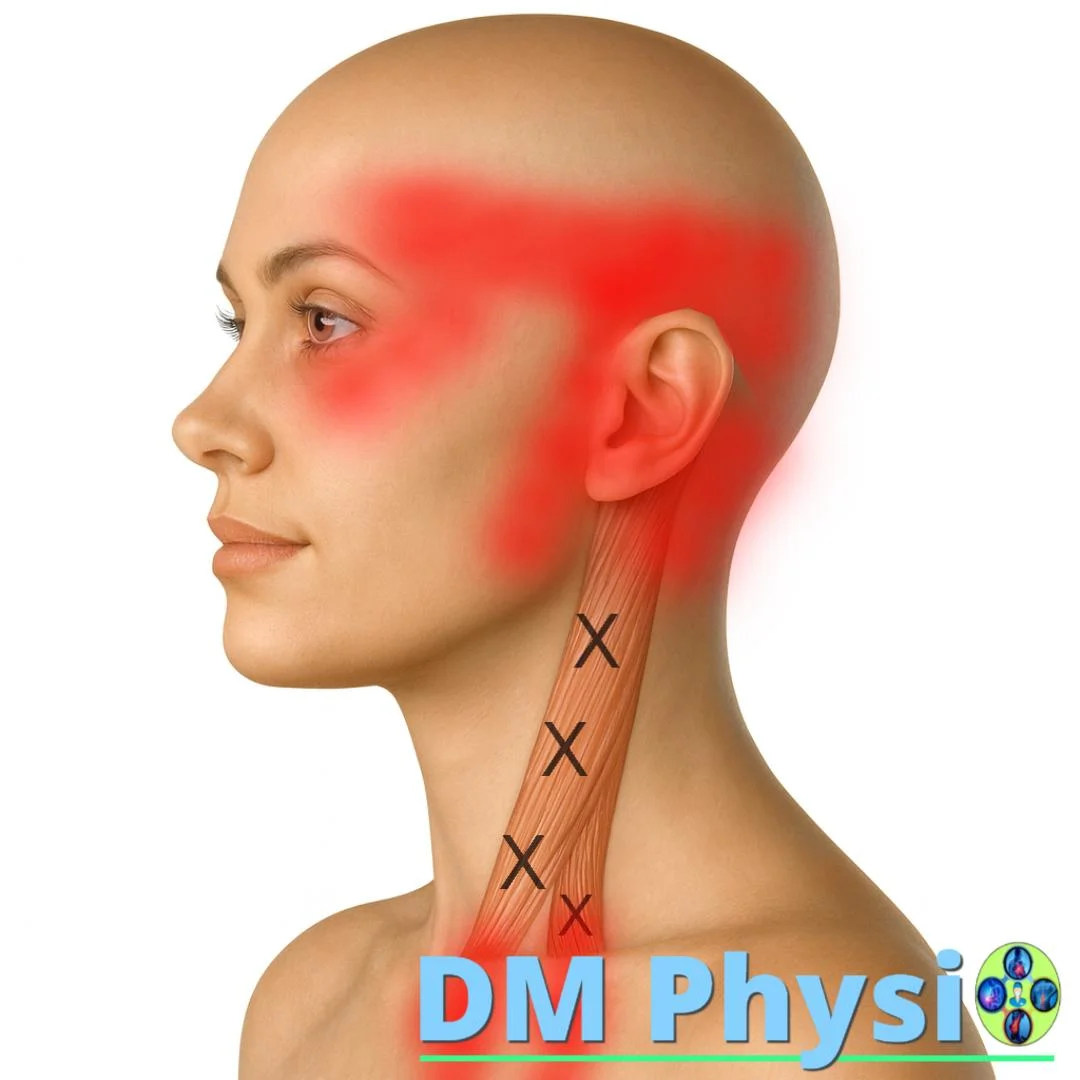
Anatomy and grip
Two chapters from clavicle and manubrium; attach for the mastoid process.
Nature of the pain
- Pain in temple and forehead
- Behind/around the eye, sometimes dizziness
m. suboccipitales
(mm. rectus capitis, mm. obliquus capitis)
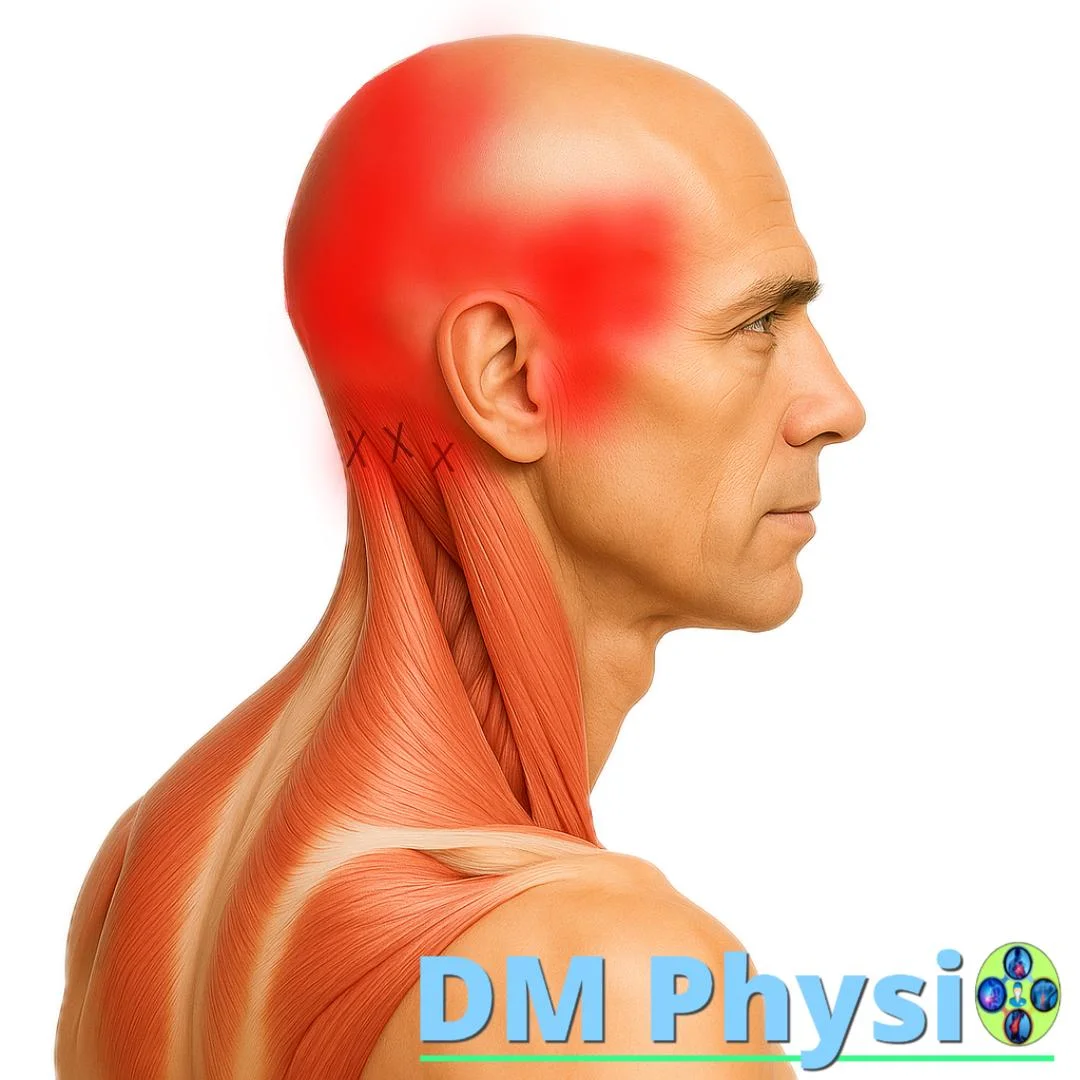
Anatomy and grip
Small, deep muscles in the base of the skull with grips on the occipital bone and upper cervical vertebrae.
Nature of the pain
- "Stabbing" in occiput radiating to temples/eyes
- Stiffness and tension in the neck
How is temple pain managed?
A combination of relaxation, rebalancing and habits for long term effect.
1) Deactivation of spasm and trigger points
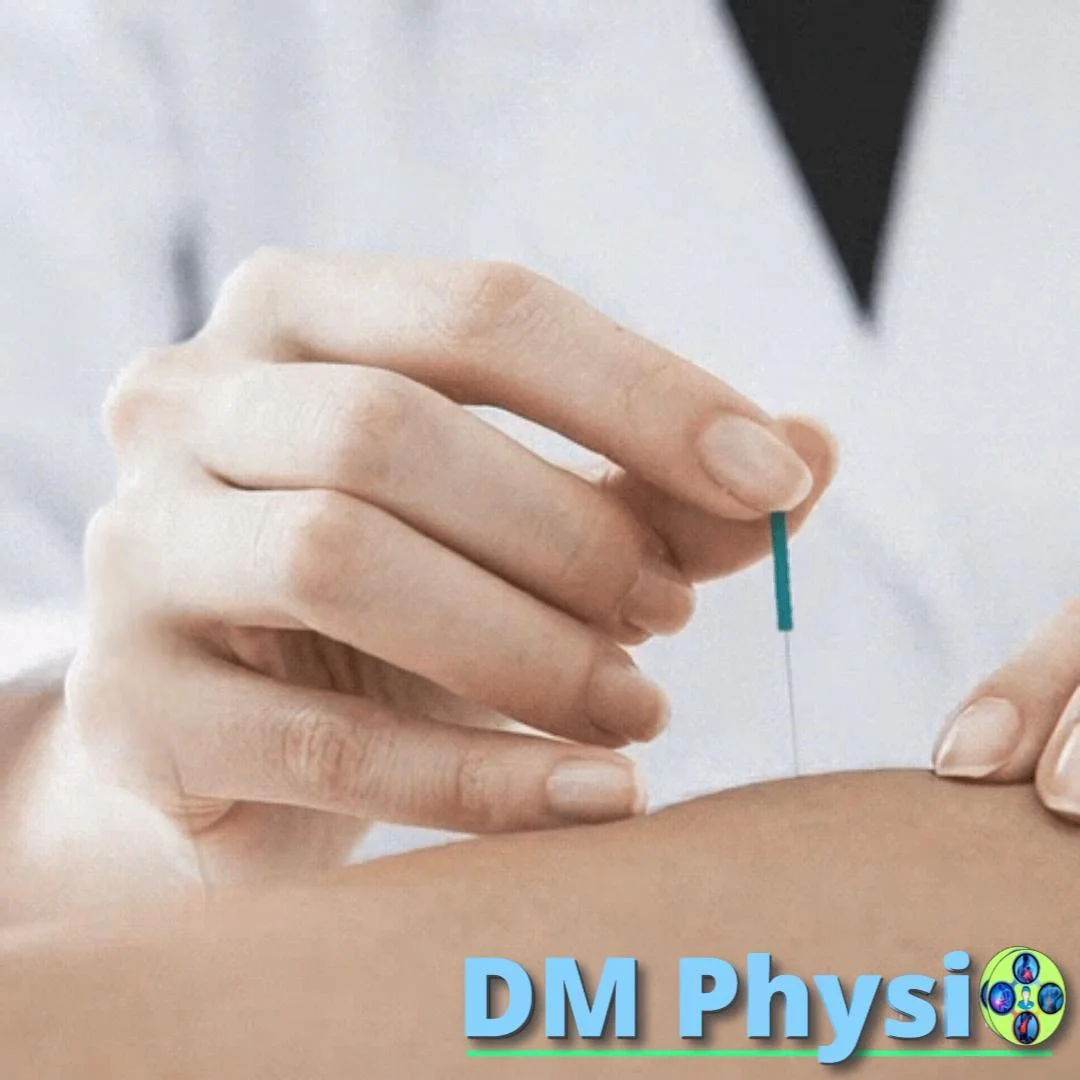
Manual techniques for temporalis/masseter, mobilization of the TM joint, work on SCM and suboccipital muscles. If needed: dry needling for a quick analgesic effect.
2) Rebalancing and stabilization
Activation of deep neck flexors, blade stabilizers, exercises for jaw/tongue control (position of the tongue towards the palate, neutral bite). Breathing patterns for tone reduction.
3) Habits and prevention
Ergonomics (screen at eye level, forearm support), stop squeezing (signals during the day), alternate sides for chewing, relaxation techniques, back/side sleep with neutral neck. At night bruxism – discussion of tire with a dentist.