Patellofemoral syndrome (pain behind the kneecap)
Pain around or behind the kneecap most often comes from poor load distribution – the quadriceps work overtime, the muscles of the hamstrings and gluteal muscles do not contribute enough. The result is overstressed patellar tendon.

What is patellofemoral syndrome?
This condition causes pain at the front of the knee, usually around or behind the kneecap. Most often, the problem is not the kneecap alone, but how the knee, hip and foot share load when walking, squatting or going down stairs.
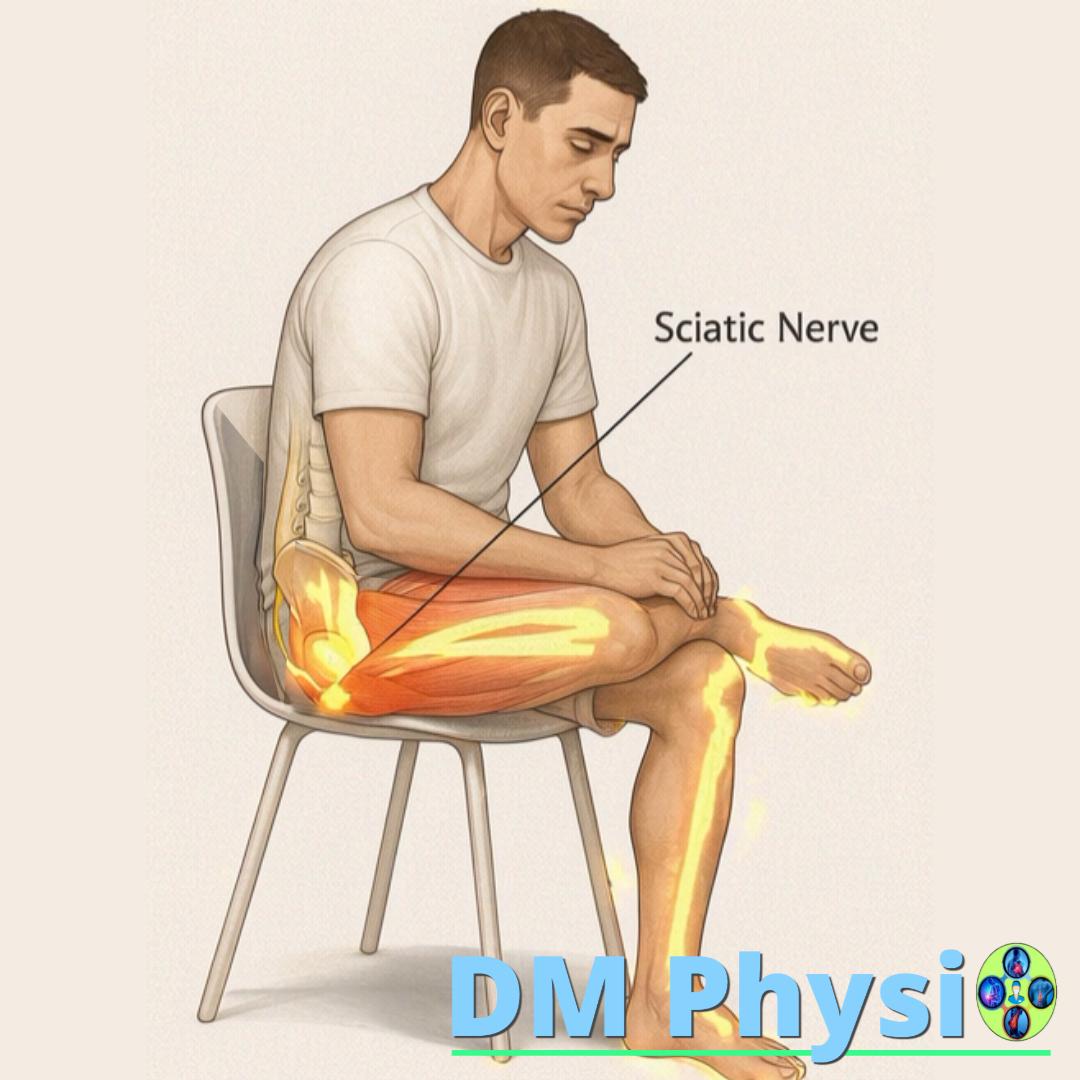
With prolonged sitting, the hamstrings and gluteal muscles may become less active. The quadriceps then take more of the load and can pull harder through the patellar tendon. Over time this may irritate the tendon and increase pain at the front of the knee.
Typical symptoms: pain when squatting, going down stairs, after sitting for a long time, when running or jumping; rubbing or cracking sensation around the kneecap; morning stiffness in front of knee.

Why is the patellar tendon overstretched?
The key is in muscle balance and the manner of loading during daily movements.
Hyperactive quadriceps
When the hamstrings and buttocks are weak, the quadriceps take over their job. It pulls harder on the patellar tendon, especially at squatting, going down stairs and walking down. Result: the tendon is overloaded and over time it becomes inflamed.
Underactive hamstrings and gluteal muscles
Prolonged sitting can make the hamstrings and gluteal muscles contribute less during movement. The body then compensates with the quadriceps, which can increase load at the front of the knee.
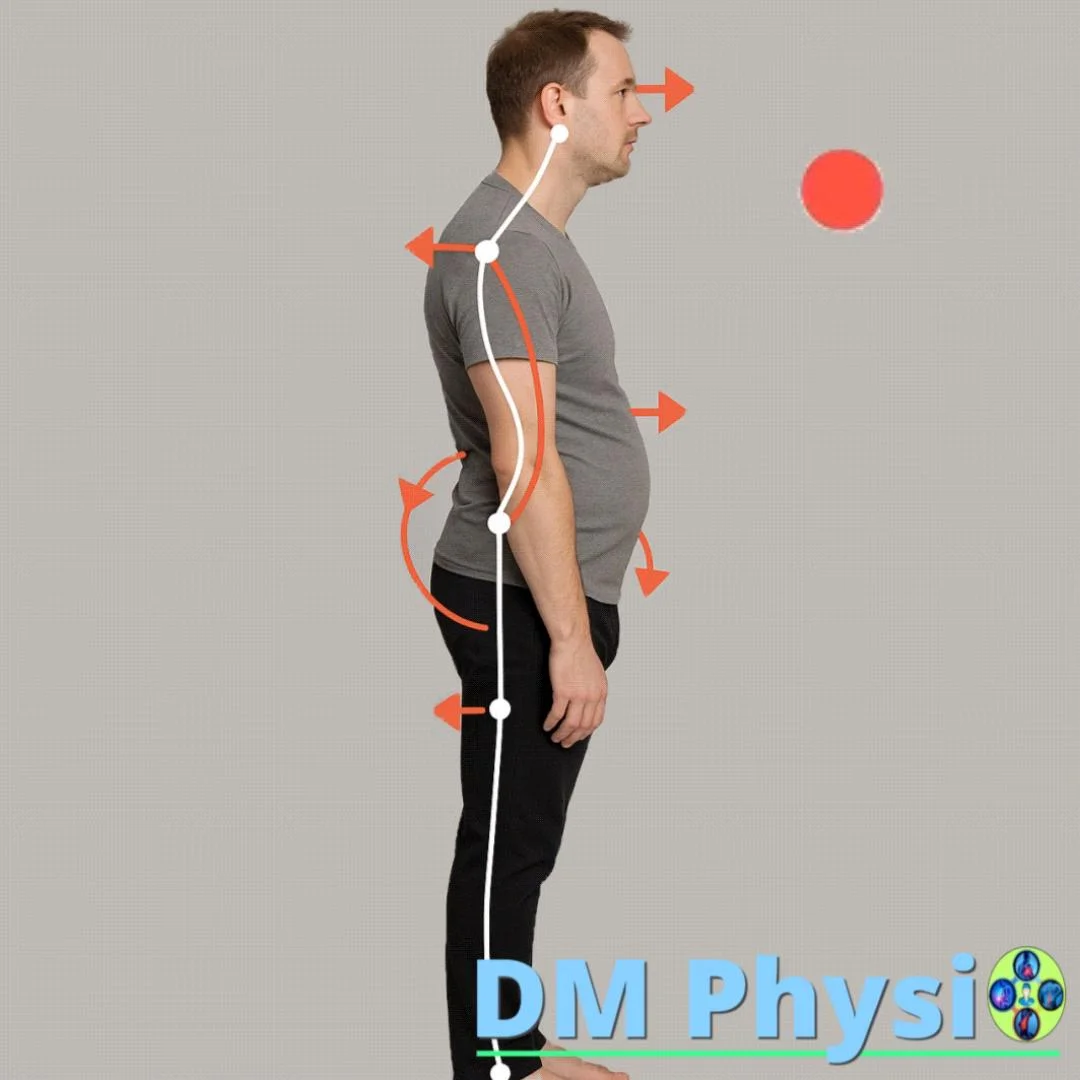
Shortened external rotators
Tight external hip rotators can turn the hip outward and shift weight toward the outer edge of the foot. This may overload the outer part of the quadriceps (vastus lateralis), pull the kneecap slightly outward and irritate the patellofemoral area. Correcting the pattern can reduce pressure over time.
Key rule: to soothe the inflammation of the patellar tendon, do not aggressively stretch the quadriceps. Load the opposing muscles instead - the hamstrings and gluteal muscles. This can reduce quadriceps overactivity and lower the pull through the tendon.
1) Hyperactive quadriceps
When the hamstrings and buttocks are weak, the quadriceps take over their job. It pulls harder on the patellar tendon, especially at squatting, going down stairs and walking down. Result: the tendon is overloaded and over time it becomes inflamed.

2) Underactive hamstrings and gluteal muscles
Prolonged sitting inhibits the muscles of the back thighs and buttocks - they "turn off" and do not help with movement. The body compensates with the quadriceps and all the load falls on the front of the knee.
3) Shortened external rotators
Tight external hip rotators turn the hip outward → we step more on the outer edge of the foot → the outer head of the quadriceps (vastus lateralis) gets overloaded and pulls the kneecap outward → irritation/inflammation in the patellofemoral area. The pattern correction immediately reduces the pressure.

How does physical therapy help with patellofemoral syndrome?
The approach has three steps: reduce overload, activate the muscles that are not contributing enough, and build better control for daily movements.
1. Relaxing the quadriceps
Through manual techniques and therapeutic massage we reduce the tension in the quadriceps and around the kneecap. The goal is to remove the excess pull on the patellar tendon and reduce pain.
2. Stimulation of the hamstrings and buttocks
We use neuromuscular stimulation , to help activate the hamstrings and gluteal muscles. This reverses their role in squatting, standing and walking so that the quadriceps no longer have to take over the whole movement.
3. Strengthening and training of movements
After activation, we move on to strengthening and training correct motor patterns. Thus, the load is distributed more evenly, the pull on the patellar tendon is reduced and the knee works more softly when squatting, walking and going down stairs.
What result to expect: less stress on the patellar tendon and more centered gliding of the kneecap, more stable knee in daily movements and smoother squatting/descending stairs with less sharp pain. The goal is for the quadriceps to stop dominating, the hamstrings and buttocks to be actively involved and the load to be distributed more balanced.