Torn ligaments in the knee
When a knee ligament is injured, a "pop" may be felt or heard, followed by swelling and a feeling that the knee may give way.

Relationships: what are they?
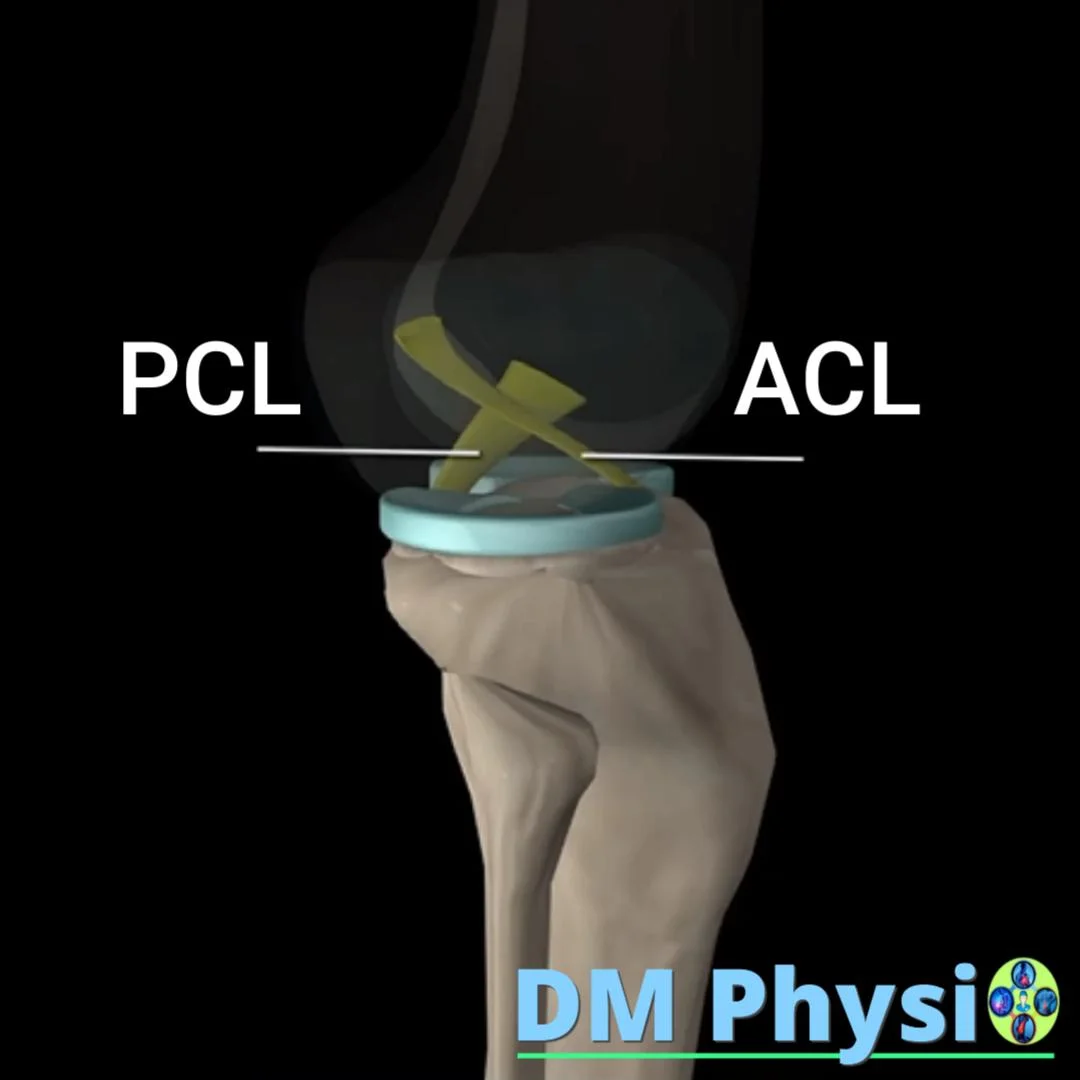
The ties are strong and elastic bands of collagen fibers, which connect the bones in the knee. They work like natural 'seat belts' - limiting excessive movement and keeping the joint stable. They also contain nerve endings that signal the brain and muscles when to kick in to protect the knee.
The most important connections are cross- front and rear, which control back and forth movement and rotations, and collateral, which keep the knee from bending inward or outward. When the muscles around the joint are weak or slow in their reaction, the load falls entirely on the ligaments, which can cause them to stretch or tear.
Healthy relationships depend not only on their own endurance, but also on muscle stability around the knee. Well-trained muscles act as a "shield" that protects the ligaments with every movement.
How are relationships most often broken?
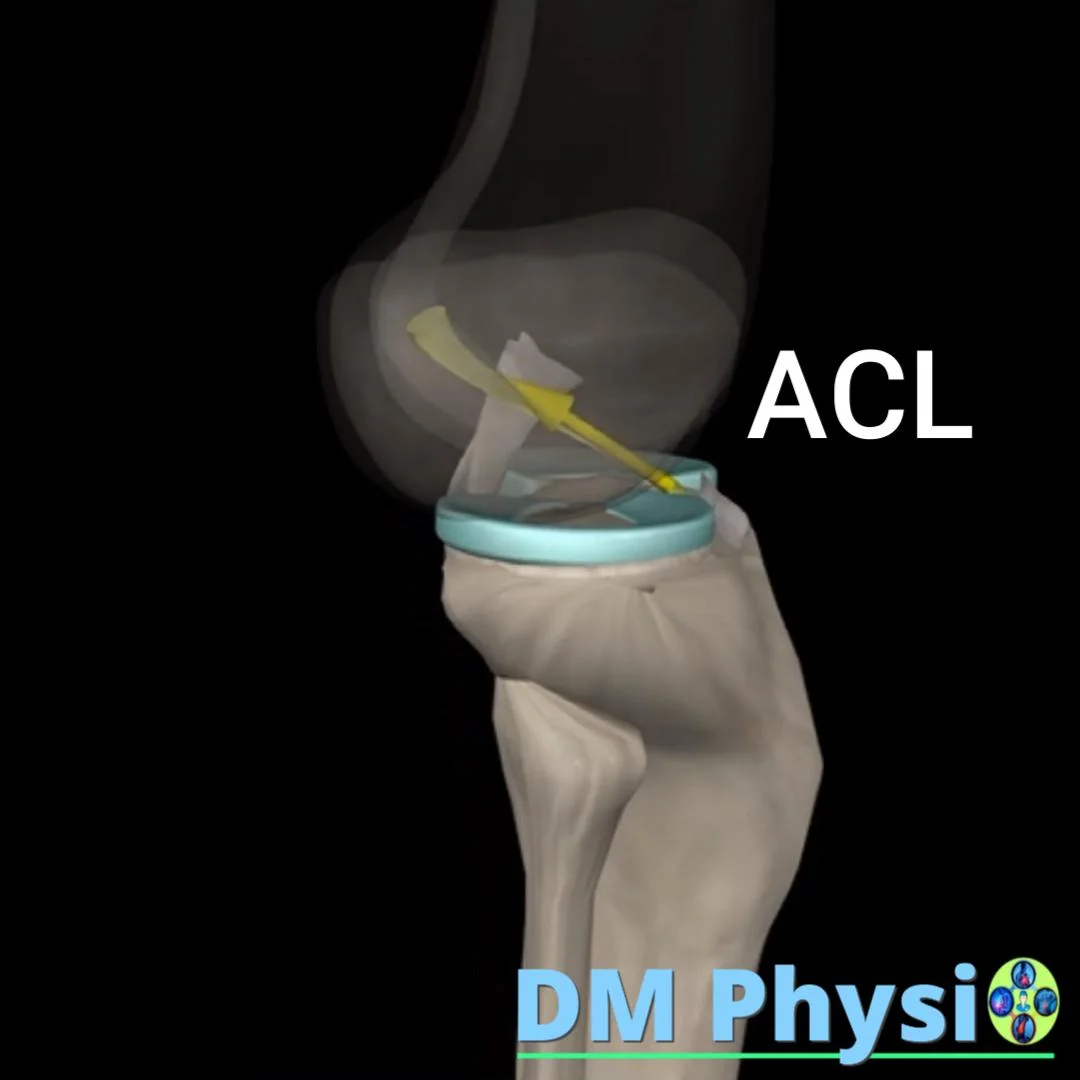
Anterior Cruciate Ligament (ACL)
Most common in sports: sudden change of direction or landing from a jump. The lower leg and thigh rotate in opposite directions, and the muscles do not "catch" in time. So all the stress falls on the ACL and it tears. There is often a "pop" and rapid swelling.
Posterior Cruciate Ligament (PCL)
Most often at a direct hit to the lower leg (e.g. in case of an accident – impact on the dashboard) or falling on bent knee. The lower leg is pushed back and the PCL is injured.
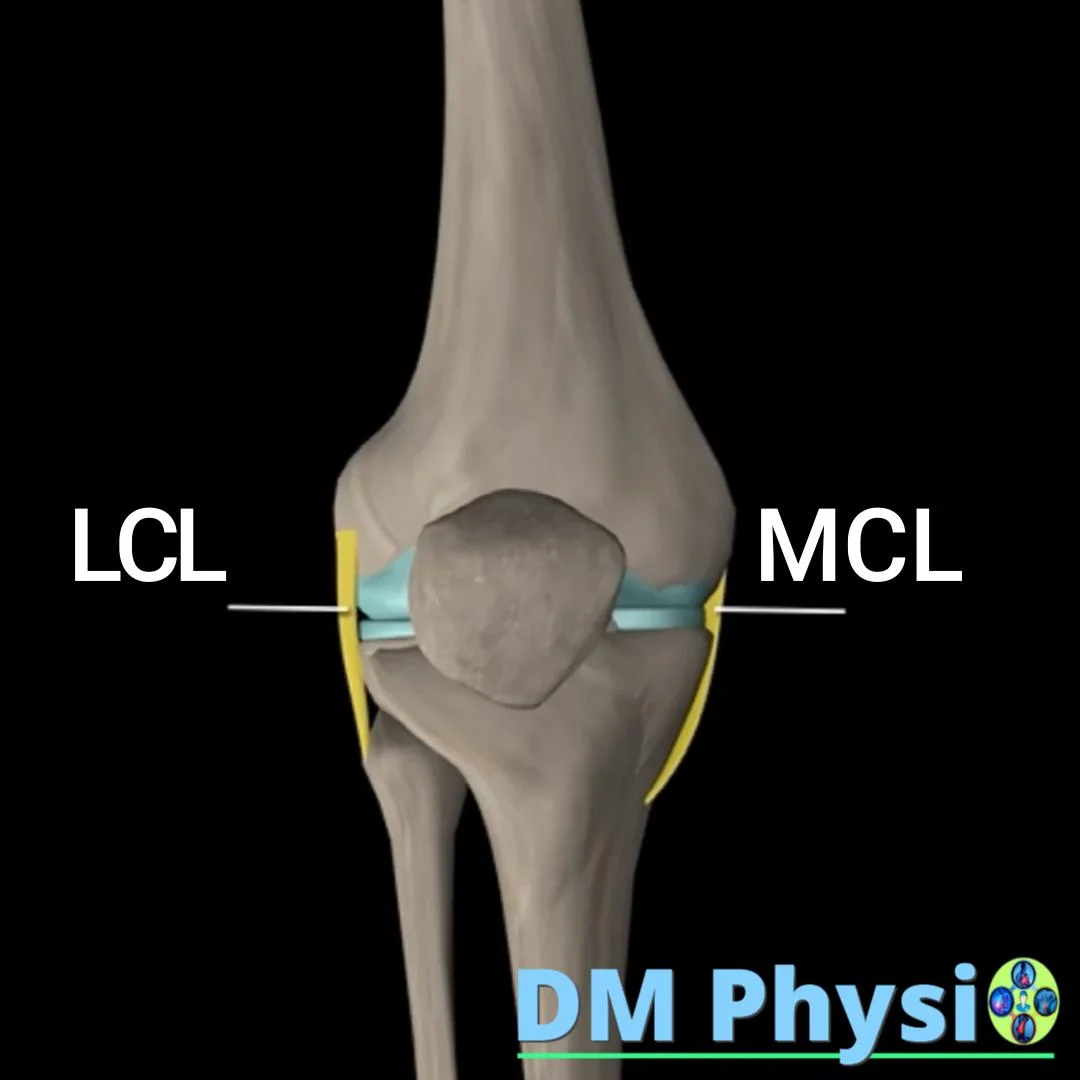
Collateral Ligaments (MCL / LCL)
When the knee curve sharply inward or outward (on contact or slipping). The ligament is overstretched and inflamed/torn. It is often combined with other injuries.
Symptoms to watch for: "pop", rapid swelling, instability ("the knee runs"), pain when turning, difficulty going down stairs.
1) Anterior Cruciate Ligament (ACL)
Most often in sports - a sudden change of direction or landing from a jump. Opposite rotation of hip and lower leg, delayed muscle response and stress falls on ACL → often “pop” and rapid swelling.
2) Posterior Cruciate Ligament (PCL)
A direct blow to the lower leg (e.g. in a traffic accident - a blow to the dashboard) or falling on a bent knee. The lower leg is pushed back and the PCL is injured.

3) Collateral ligaments (MCL / LCL)
Abrupt bending of the knee inward or outward (contact/slip). The ligament is overstretched and inflamed/ruptured; there is often collateral damage.
Physiotherapy - before and after surgery (plain and simple)
Our goal is a stable knee, without pain, with confidence in movement - with or without surgery.
Before surgery (PREHAB)
Why? The more prepared the knee goes in, the easier it comes out of surgery.
What we do: we take down the swelling and the pain, we return the full erection and the good folding,
we "wake up" the quadriceps and buttocks, learn to walk with a "soft" knee.
Result: faster and safer recovery afterwards.
Early period after surgery
Purpose: protection of the new joint, control of pain and swelling, smooth movement.
We use gentle mobilizations, gentle activation exercises, neuromuscular stimulation for
"waking up" of the quadriceps and normalizing the gait (no limp).
Return to strength, confidence and sport
Step by step we add strength, balance and coordination - squats, lunges,
glute and hamstring work, then jumps and changes of direction.
Without surgery: we build muscles to take over the stabilization and keep the damaged connection in everyday life and sports.
Important in brief: Strong, well-coordinated muscles support the knee and unload the connections. This is the best prevention before trauma and the safest path after trauma. Operation is recommended if the goal is active sport with sudden changes of direction and jumps.